
Stereotactic neurosurgery is a "minimally invasive" sort of surgery. In other words, it can be used to reach inside the most inaccessible areas of the brain, without resorting to extensive opening of the skull and unnecessary and undesirable destruction of normal brain areas lying above the target, as is often the case with conventional, invasive surgery of the brain.
The stereotactic approach has represented a remarkable technical progress in neurosurgery. It has precise indications and many advantages, and has innovated the therapy of several focal diseases of the brain (that is, when the disease is being caused by a pathological alteration which can be located in a particular and restricted area of the brain), such as brain tumors, congenital vascular disorders, Parkinson's disease, epileptical foci, etc.
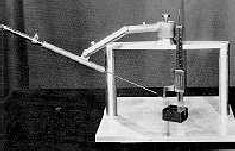 |
Stereotactic surgery was made possible by the invention
of an apparatus by the British surgeon Victor Horsley,
in the beginning of this century. Known as the Horsley-Clarke
apparatus, it allows the precise
positioning of the patient's head inside a geometrical coordinates system, so that each structure inside the brain
can be reached from the outside. The neurosurgeon needs only to make a small opening in the patient's skull, under local anesthesia. Then, a thin straight probe is introduced into the brain, and using a remarkably precise system of geometrical coordinates, it is targeted onto the internal structure of the brain which the neurosurgeon wants to remove. |
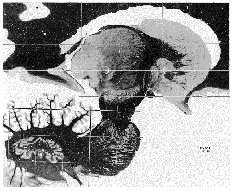 |
An atlas of the brain maps out these structures for the neurosurgeon. Depending on the system which is used (there are many variations), each brain structure can be assigned three unique numbers, or coordinates: in the rectangular, or cartesian coordinate system, they are the positions along three axes or dimensions. There is also a polar coordinate system, which uses a combination of angles and lengths to specify the coordinates of the brain structures. Modern stereotactical surgery was pioneered by the Swedish neurosurgeon Lars Leksell, who invented an apparatus suitable for clinical use in humans, which is still in use today. |
 |
To perform the surgery, first the surgeon calculates the exact point where the skull will be opened. With the help of a hand or motor-operated drill, a small aperture bore is made onto the exposed bone. The patient is under local anesthesia, most of the time. |
 |
Then, the head of the patient is firmly placed into the stereotactic apparatus, by using pre-determined points of reference in the bone structures of the head. |
 |
Now a straight probe, which can be a metallic electrode or a hollow cannula, is attached to the stereotactic apparatus and inserted into the brain, passing through the hole, until it reaches the calculated spot in the middle of the brain. Using x-rays taken with a portable apparatus, it is possible to visualize where the tip of the probe is located, and increase the precision of its location. The lesion of a small area inside of the brain can be performed by passing a direct or an alternating electrical current at the probe's tip (it is electrically insulated all along its shaft, except at the tip, in contact with brain tissue). Direct current destroys tissue by electrolytic action, while alternating current destroys by heat coagulation (by using a frequency in the radio range, it heats the tissue up to 70 degrees Celsius, very much like in a microwave oven). |
 To Know More
To Know More
Picture Credits: Mark, V.H. and Ervin,
F.R.. "Violence and the Brain", Harper & Row, New York, 1970.; Schaltenbrand and Wehre,. "Stereotactic
Atlas of the Human Brain".
From: The History of Psychosurgery
Author: Renato
M.E. Sabbatini, PhD
Source: Brain
& Mind Magazine, June 1997
![]()

12 of 15